
Do I Need Medication for Life Once I Start? | PsyConnect
Worried psychiatric medication means a lifetime commitment? Dr. Mahendra Singh Uikey explains how treatment duration actually works in India.
PUBLIC MENTAL HEALTH
"If I start, will I be on this forever?" It's one of the most common questions I hear in a first consultation — often asked before a diagnosis has even been discussed. The fear of lifelong dependence keeps many people from starting treatment they need, or pushes them to stop a medication on their own once they feel better. Both choices can do more harm than the medication itself. This article explains how treatment duration is actually decided, and why "starting" and "forever" are not the same thing.
The Short Answer
No — for most people, psychiatric medication is not a lifetime sentence. Duration depends on the specific condition, how many episodes you've had, and how you respond to treatment. Some people take medication for 6–12 months. Others, particularly with recurring or chronic conditions, may need longer-term or maintenance treatment — similar to how some physical health conditions are managed long-term. The decision is individualised, not automatic.
Why This Fear Is So Common in India
Several cultural and structural factors feed this worry:
Stigma around "always being on something" — equating ongoing treatment with permanent illness or weakness
Family pressure to stop once symptoms improve — "you look fine now, why still take tablets?"
Confusion with addiction — psychiatric medications for depression and anxiety are not addictive in the way people fear, though they should always be tapered under supervision
Past experience of abrupt discontinuation — stopping without medical guidance, leading to relapse, which gets remembered as "the medicine not working" rather than "stopping incorrectly"
Understanding these patterns helps separate the genuine clinical picture from inherited fear.
What Actually Determines Treatment Duration
1. The specific diagnosis
Different conditions have different evidence-based timelines:
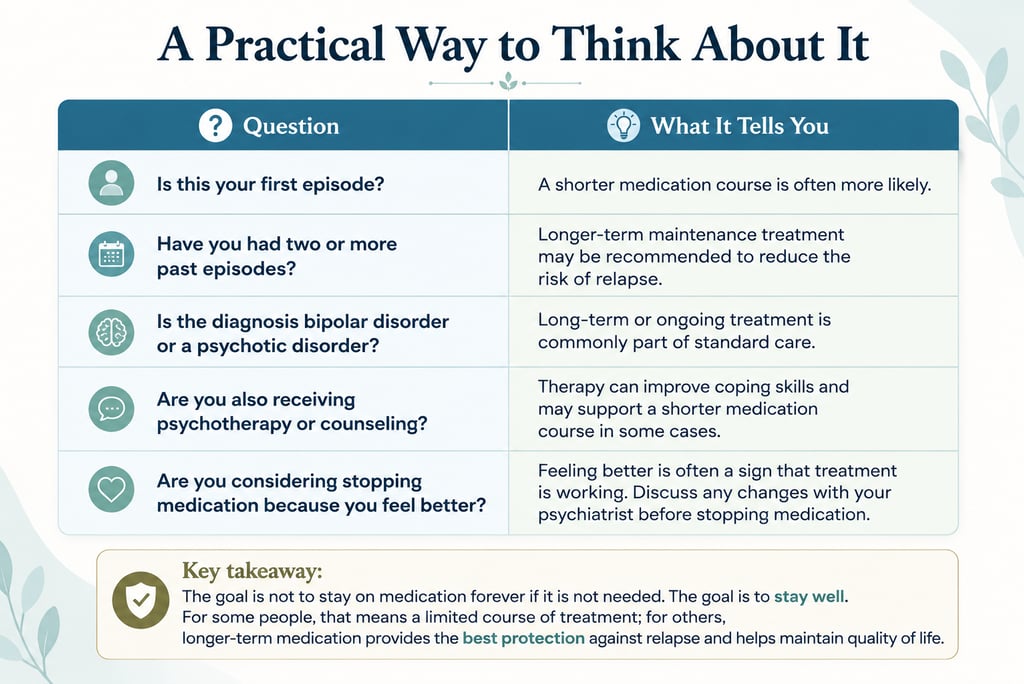
First episode of depression or anxiety — typically treated for 6–12 months after symptoms improve, then reassessed
Recurrent depression (multiple past episodes) — longer maintenance treatment is often recommended to reduce relapse risk
Bipolar disorder — usually requires longer-term mood stabilisation, as the underlying pattern tends to recur
Schizophrenia and psychotic disorders — typically need sustained treatment to prevent relapse, with duration individualised
Situational anxiety or adjustment-related symptoms — may only need short-term support alongside therapy
2. Number of past episodes
Each depressive or manic episode increases the statistical likelihood of another one. This is why a first episode and a fourth episode are often treated differently — not because the person is "more broken," but because the evidence supports longer protection after repeated episodes.
3. How you respond and how it's tapered
Even when medication is time-limited, stopping is a process, not an event. A psychiatrist tapers the dose gradually and monitors for early signs of relapse. This is medically different from "being on it forever" — it's structured discontinuation, planned in advance.
4. Severity and impact on functioning
More severe or functionally disabling episodes generally warrant a longer stabilisation period before any tapering is considered.
What Happens If You Stop on Your Own
This is one of the most important safety points in this article. Stopping psychiatric medication abruptly, without medical guidance, can cause:
Discontinuation symptoms that are sometimes mistaken for "relapse" or "the illness coming back"
Genuine relapse of the underlying condition, sometimes more severe than the original episode
Loss of the chance for a planned, gradual taper that minimises both risks above
If you're considering stopping — whether because you feel better or because of side effects — the right step is to discuss it with your psychiatrist, not to decide alone. A planned taper protects you in a way that stopping abruptly cannot.
Medication Alone Isn't the Only Path
For many people, the goal isn't "medication forever" — it's "medication for now, while other tools are built." Structured psychotherapy (like CBT), lifestyle changes, and relapse-prevention planning can sometimes allow for a shorter medication course or a lower maintenance dose over time. This is part of why psychiatrists and psychologists working together — medication alongside therapy — often produces better long-term outcomes than either alone.

The Bottom Line
Starting psychiatric medication is not a lifetime commitment made on day one — it's the beginning of a plan that gets reassessed as you go. The right question isn't "will I be on this forever," but "what does the evidence say for my specific situation, and how do we revisit this together over time." That conversation is something only a psychiatrist who knows your full history can have with you.
This article is written for informational purposes and does not constitute medical advice. Please consult a qualified psychiatrist for personalised diagnosis and treatment.
Consult Dr. Mahendra Singh Uikey
Dr. Mahendra Singh Uikey is an AIIMS-trained Consultant Psychiatrist providing evidence-based psychiatric care online and in-person across Delhi-NCR.
If you're unsure whether medication is right for you — or worried about how long treatment might last — a consultation can help clarify your specific picture before any decision is made.
This article is written for informational purposes and does not constitute medical advice. Please consult a qualified psychiatrist for personalised diagnosis and treatment.
© PsyConnect | Dr. Mahendra Singh Uikey | care@psyconnect.in
Contact
Reach out for support and appointments
care@psyconnect.in
©2026. All rights reserved.
Confidential. Evidence-based. Ethical psychiatric practice.
If you are in crisis or having thoughts of self-harm or suicide, please reach out right away. Support is free, confidential, and available 24/7.
Tele-MANAS (Government of India): 14416 or 1-800-891-4416 — available in English and 20 regional languages
ICall (TISS): 9152987821 — counselling support by trained professionals
AASRA: 9820466726 — 24/7 crisis support
Emergency: Contact your nearest hospital or call 112
IMMEDIATE SUPPORT
+91 82877 12625 (Reception)